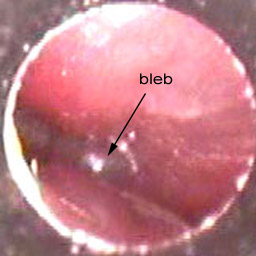
Ear Attic Defect

Eardrums Seen In 8 Conditions Normal Eardrum Acute Otitis Media Perforation Small Perforation Attic Perforat Otitis Otitis Media Health Assessment Nursing
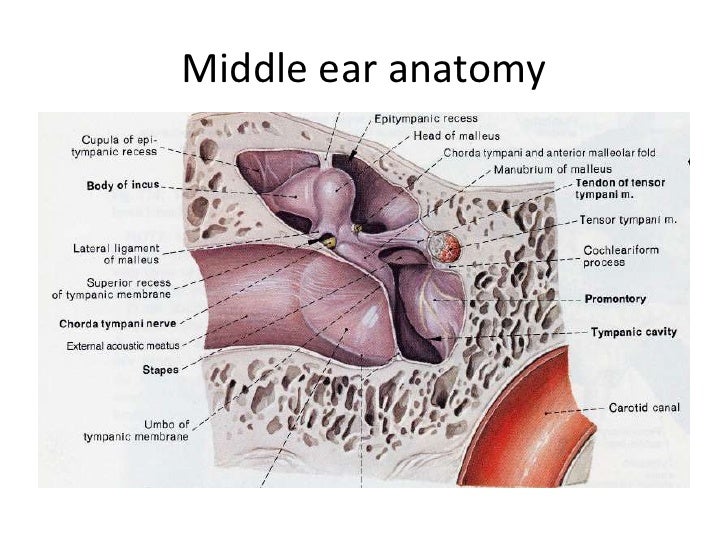
Unit Four Middle Ear Disease Diagnosis

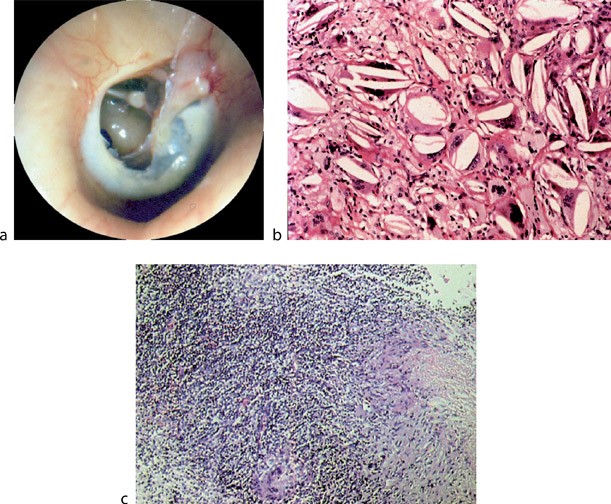
Cholesteatoma Stanford Children S Health

Transcanal Endoscopic Butterfly Island Cartilage Tympanoplasty Cartilage Island Grafting
Atticotmy
Https Thieme Connect De Products Ebooks Pdf 10 1055 B 0039 171429 Pdf

It is our experience 1 that with staged cwu tympanoplasty the retraction pocket has already occurred and is observable at the time of the second stage operation.
Ear attic defect.

Zenith 7s 558 1940 Vintage Radio Antique Radio Old Radios

Hearing Disorders Chapter 20 The Cambridge Handbook Of Communication Disorders

Vintage Mouse Figurine Vintage Mouse Knick Knack Mouse Mouse Eating Cheese Figurine Josef Originals 0 738 Wide Eyes Brow Vintage Collectibles Figurines

Pin On My Posh Picks

Identify The Signs Hearing Problems Hearing Health Hearing Impairment

Marx Linemar Henry Eating Candy Windup Toy Vintage Toys Retro Toys Classic Toys

Left Ear View Of The Tympanic Cavity From The Eustachian Tube 1 Download Scientific Diagram

Getting Started In Endoscopic Ear Surgery Sciencedirect

Vintage Bunny Plush Rabbit Dakin Life Like Stuffed Animal Brown Tan Easter Dakin Korea 1986 In 2020 Bunny Plush Vintage Bunny Vintage Plush

Cholesteatoma London Ear Clinic

Vintage Louis Marx Roll Over Cat Wind Up Tin Toy W Box Ebay Igrushki

Time Out Area Study Area For The Easily Distracted Student With Some Of Those Defective I E Student Damaged Headphones As Ear Mufflers Small Space Office

42 Dog Ear Picket Fence Backyard Fences Wood Fence Design Picket Fence

Image Result For Scutum Erosion Facial Nerve Eustachian Tube Dysfunction Middle Ear
Middle Ear Disease Chronic Springerlink

White Donkey And Cart Planter 1080 With Images White Donkey Vintage Planters Planters

Vintage Anson Gold Tone Woven Rope Design Cufflinks Cufflinks Rope Design Woven

Pin Pa Figurines
Https Encrypted Tbn0 Gstatic Com Images Q Tbn 3aand9gcshxigp1cp Lksw5eyrjfubeo7r11ccyg1sj86hrxlmpnhx Awv Usqp Cau

Bunny Animug Easter Eggs In Bottom Of Mug Hidden Surprise Inside 12oz Peek A Boo Easter Eggs Easter Bunny

The Radiology Assistant Temporal Bone Anatomy 2 0 Cabeca E Pescoco Pescocinho

Minimal Decor Pieces By Aksanaoneofakind In 2020 Recycled Wood Sophisticated Decor Beautiful Decor
Https Www Bonalive Com Wp Content Uploads 2019 07 Mastoid Surgery Bonalive 9 100010 Pages Pdf

Vintage Oval Earrings Turquoise Blue Enamel Shiny Gold Inlaid Angled Stripes Post Earrings 1980s Big Bold Ear Red Earrings Vintage Style Earrings Oval Earring
Source : pinterest.com
